
REGISTRIES/COHORTS IN RHEUMATOLOGY
When requested to pen this article, I wondered aloud.... What am I going to do? To my utter surprise, I found a voluminous content, which was difficult to document. The pains taken initially to collect the necessary data be it demographic, clinical, genetic associations, laboratory abnormalities, biorepositories, course of the disease with longitudinal follow-ups, complications, comorbidities, treatments-conventional vs newer ones,especially biologics and JAK inhibitors, their complications, collaborative studies and later advancements in entering data, web based etc.,has made us look up in awe, at the horizon.
REGISTER…. What is it?
Could very well be a sheath of papers, diary, notebook etc compiled with important information-birth, death, marriage, attendance etc.Surely, it is a memorable document.
A REGISTRY….(patient or clinical) is defined as “an organised system that uses observational study methods to collect uniform data to evaluate specified outcomes for a population defined by a particular disease, condition or exposure and that serves predetermined scientific, clinical or policy purpose(s).”(1)
There are different types of registries:
(a) Disease based
(i) Cross sectional-Ibero-American registry
(ii) Longitudinal cohort (fixed cohort of all cases-SPARTAN)1
Inception: Early cases, eg. DESIR, ASAS
Dynamic: Continuous inclusion, eg. CORRONA
Historical: eg. OASIS
Combined registries: eg. PSOAS, PULSAR and SPARCC.
(b) Treatment based- As is used in phase IV studies, eg. BIOBADASER, DANBIO
There are also cost effective evaluative registries focussed on academics (SpA Net) or like the Korean registry focussed at the national government level.
However, the reach of registries in terms of being accessed or read is far lesser than concentrating on individualised original studies or drug trials. The amount of labour that goes into the making of even the simplest of registries cannot be expressed in mere words. It involves various steps, starting from the formation of an organising committee which decides the endpoints (2). Then Who will be the leader? Who will take care of funding, data collection, followed by recruiting trained and committed investigators, monitoring, choosing the criteria, quantification etc.
- Quantification requires standardised protocols which are already validated and help to reduce interobserver variability.
- The appropriate sample size should be reached.
- Realistic end and data points should be achieved within the budget.
- Adherence to the study should be strictly followed.
- Upfront dealing should be done for missing data compilation statistics (which should be useful for finding out the reasons and rectifying them-thereby helping the patients and future studies)
- The availability of data dictionaries help in maintaining the consistency, uniformity and accuracy.
Coding manuals are a must (2).
They look into different diseases in different populations, for complete demography, manifestations, complications, treatment, comorbidities, risk factors, habits, family involvement, phenotypes, age differences etc. They have more inclusion and less exclusion criteria, widening the horizon of their reach; especially for rare diseases (2). Initially they were manual, but it is a different scenario today. With the advent of online electronic facilities collaborations have become the order of the day.
Some of the well known rheumatology registries are disease based registries for rheumatoid arthritis (RA), spondyloarthropathies (SpA), systemic lupus erythematosus (SLE), Scleroderma (SSc), Myositis (IIM), Vasculitis etc. Registries which have revolutionised today’s scenario are the treatment based registries, like the “BIOLOGICS” registries. Innumerable are the data which are unbiased, starting from safety, efficacy, dosages, frequency and route of administration, cumulative dose, duration, cost factors, adherence and side effects, developing and updating classification and diagnostic criteria, outcome measures, collaborations, comparisons and what not.
Let us now peep into some of these registries.
SPONDYLOARTHRITIS (SpA):
ASAS Cohort: Assessment of Spondyloarthritis International Society
This served the purpose of validation of the new classification criteria for axial SpA, where the radiographs were compared with active inflammation on pelvic MRI. This should pave the way for reduction in MRI rates or maybe power doppler studies or even nanotechnology.
CORRONA (Consortium of Rheumatology Researchers of North America) JOHN HOPKINS-40,000 patients
This assesses longitudinal outcomes in patients with SpA (Ankylosing Spondylitis and Psoriatic arthritis are inclusions). It is a dynamic registry including comorbidities, also providing information for treatment decisions. It has a large data set. Maybe it can be expanded to other countries in a collaborative effort thereby helping to compare their details and thus providing a base for study of some or different drugs in varying doses for varying durations.
IBERO – American Registry-3439 patients
It includes 100 universities – from RESPONDIA and REGISPONSER (Spain) studies showing large clinical differences. They can get involved in discovering the genetic associations.
OASIS (Outcome Assessment in Ankylosing Spondylitis International Study)
This is a longitudinal observational historical cohort, which used a comparison cohort for addressing radiographic progression in most of the anti-TNFalpha trials. It is a decade long follow cohort and thus a revolutionary one too. Maybe they can be combined with other drugs as well.
PSOAS (Prospective Study of Outcome in Ankylosing Spondylitis)-961 patients
This is an NIH longitudinal study since 2002 with two-thirds of patients still under follow-up. It is very comprehensive and with a methodical follow-up assessing clinical, psychological, demographic, including a collection of genetic, serological and radiological details.
Korean SpA Registry Cohort
This is an ongoing longitudinal observational study that also includes BASFI.
SPARCC (SpA Research Consortium of Canada)-2028 patients
This is a transdisciplinary approach addressing genetic susceptibility, developing and validating clinical and imaging outcomes to assess disease activity and structural damage, response to treatment, quality of life and disability. Good indices-SPARCC enthesitis index and SPARCC imaging scoring system have emerged.
PULSAR (Programme to Understand Long-term outcome in SpA Registry)-434 patients
It deals with, in addition to articular manifestations, the extra articular manifestations along with the treatment profile.
SPARTAN (SpA Research and Treatment Network)
It is a collaboration of PSOAS, PULSAR and SPARCC registries.
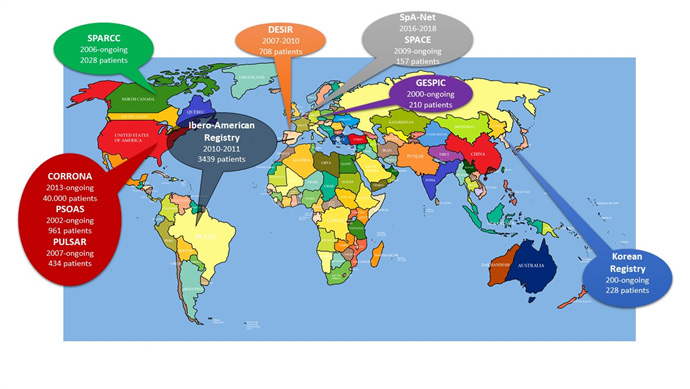
Disease based registries for SpA from across the world: Geographical distribution and basic information (1)
SYSTEMIC LUPUS ERYTHEMATOSUS
No article is complete without mentioning the JOHN HOPKINS RHEUMATOLOGY and the services rendered by them encompassing arthritis, myositis, scleroderma, sjogren’s, vasculitis and not forgetting the erstwhile “Lupus”. Their attractive online sites, whether it is the Lupus center or primer are a boon to both Lupus patients and treating physicians alike.
Lupus Family Registry and Repository (LFRR) is amazing, starting from its inception till date. It had a humble beginning in the early 1990s by John Harley at the Oklahoma Medical Research Foundation (OMRF) where multiplex pedigree families were collected, leading to the formation of the Lupus Multiplex Registry and Repository. The Repository housed data, sera, plasma, DNA, transformed B cell lines and peripheral blood mononuclear cells. Sample size being greater than 5 million data points for each sample, reaching the pinnacle, genotyping from microsatellites to single nucleotide polymorphisms (SNP). The beauty here is samples are stored in 2 places for emergency backup. CH50 is being done and also the Genome Wide Association Studies (GWAS) are performed. Follow-up and reviews are strict. More than 650,000 SNP markers have been analysed. One billion genotypes are distributed by web-based interface. However, one of the drawbacks is, there is little data on the longitudinal course of the disease.
RELESSER (The Spanish Rheumatology Society SLE registry)
It is the largest European registry, in force from 2011. Apart from details about SLE, it has addressed incomplete SLE (iSLE). Activity indices like SELENA-SLEDAI, SLICC, ACR/DI and KATZ index were used. APLA coexistence, comorbidities, refractory SLE (inefficacy of CYC, RTX, splenectomy or inefficacy of 2 or more immunosuppressives) were included. 10% of SLE were iSLE. Comparison of iSLE was done with other registries with the conclusion that iSLE does progress overtime to SLE, but with a low damage accrual rate. Its limitation is its retrospective design (4).
RHEUMATOID ARTHRITIS- LESSONS LEARNT FROM BIOLOGIC REGISTRIES
There are registries galore with BIOLOGICS flying in from all quarters, especially EUROPE, UK, USA and South Korea. Abundant data are available on switching biologics, csDMARDs vs Biologics. The lesser effects of biologics on smokers compared to non-smokers and how methotrexate has no added benefit with Rituximab. It has shown better effects of Tocilizumab and Rituximab after anti-TNF alpha failure. Tocilizumab as a monotherapy is good. Rituximab in fixed doses at fixed intervals is effective (CERRERA). The Japanese have shown that flares develop after stopping bDMARDS. Anti-TNFAlpha works well in younger patients. Anti-TNFalpha and Tocilizumab are good first-line drugs. Abatacept with csDMARDS is better than monotherapy.
The major advantage of the registries is the enormous number of patients enrolled and the recording of rare adverse events, which is not feasible in drug trials.
INFECTIONS:
The ROB-FIN registry showed that infection risk was not different from csDMARDS. The RABBIT registry showed increased susceptibility to tuberculosis with combined anti-TNFalpha with cSDMARDS. However, the incidence has reduced after the recommendations.
MALIGNANCIES:
Except for conflicting reports about individual malignant and solid tumours, the risk of others including lymphoma is reassuring.
CARDIOVASCULAR SYSTEM AND CENTRAL NERVOUS SYSTEM:
Anti-TNFalpha treatment reduces risk of coronary syndrome compared to csDMARDs. The risk of cerebrovascular accidents is reduced.
GI PERFORATION:
RABBIT recorded reduced perforation due to Tocilizumab. Perforation was due more to steroids than anti-TNFalpha.
OTHERS:
However, the BIOBADASER registry showed infections, infusion reactions, skin diseases, malignancies and autoimmune diseases due to anti-TNFalpha drugs.
BENEFITS:
Registries document the response to treatment, safety, additional and complementary information compared to Randomised Controlled Trials.
Collaborations across registries help in comparing the efficacy and safety between csDMARDS, bDMARDS, JAK inhibitors and other drugs. Collaborations provide a “BIG DATA” mine (5).
MYOSITIS:
Both clinical and patient support group registries are available. The largest is the Euromyositis one which has expanded globally through Myonet, encompassing 3000 patients. Apart from demographics, manifestations, outcome measures (IMACS), longitudinal follow-up, it has contributed to genome-wide association studies (GWAS), prognostic markers, Myositis Specific Antibodies(MSAs) and multicenter myositis drug trials including biologics. It includes the JDM as well. Large collaborations and funding are needed for further expansion (6).
SYSTEMIC SCLEROSIS:
American, European and Australian Registries exist. EUSTAR is a major well-known International online database. Collaborations with Pulmonary Hypertension example (PHAROS) will throw more insight into cardiac involvement and management strategies. Collaborations with ILD registries will also help in management. UK houses the SMART data bank (7).
VASCULITIS:
Well-known International Vasculitis Registries are the EUVAS, UKIVAS and the DCVAS (the largest international study in vasculitis). The Portuguese vasculitis registry is a web based one. Its collaboration with INFARMED ensures documentation of adverse effects of treatments(8). Most of these registries deal with vasculitides, Behcet, PAN and large vessel vasculitis like GCA.They have dealt in depth about these diseases starting from demographics, clinical manifestations, biomarkers, longitudinal follow-up, complications and response to different modalities of treatment including biologics. They have also helped in the framing of new classification and diagnostic criteria. Weightage has been given to different manifestations in these criteria. Outcome measures have also been included.
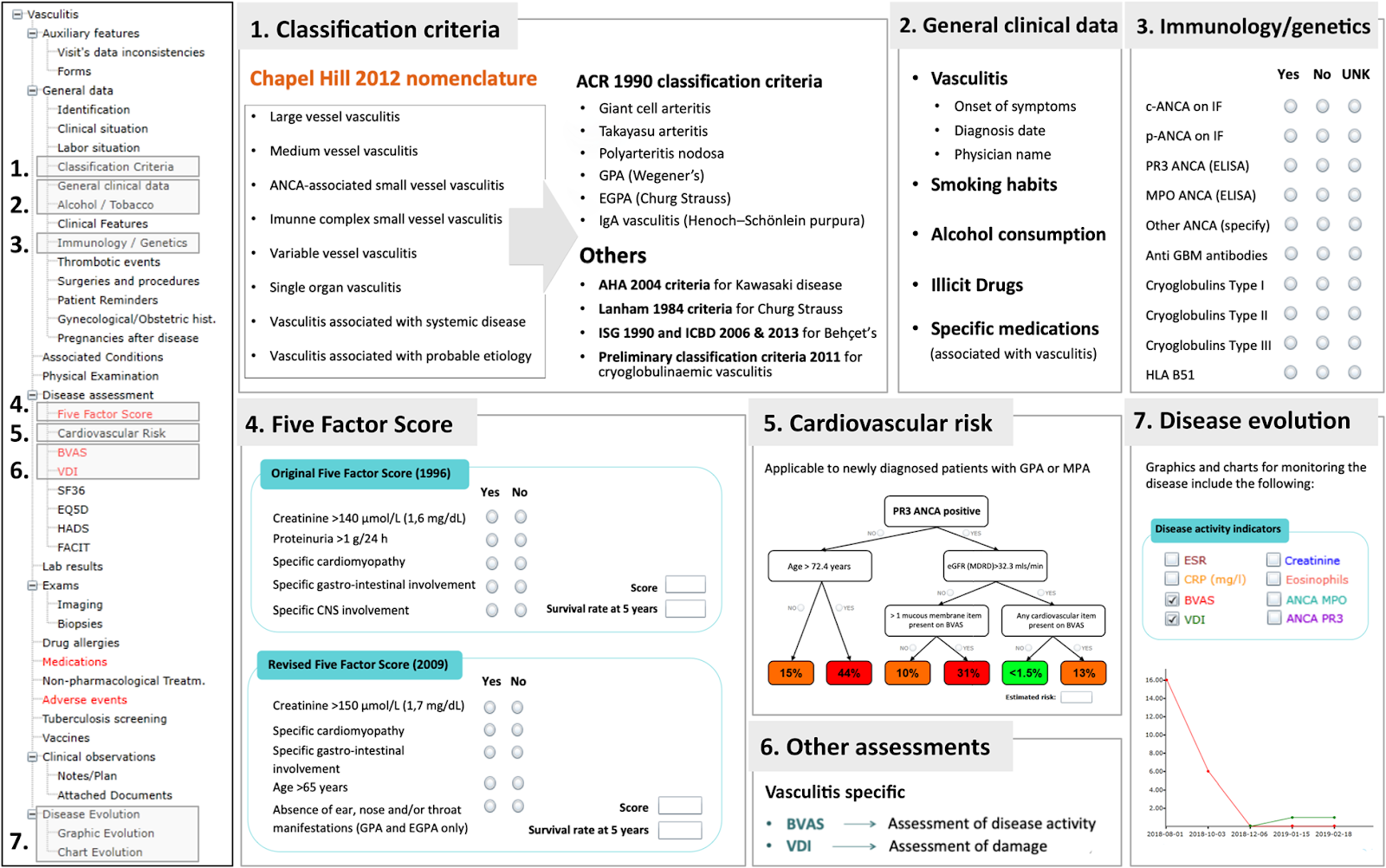
Brief summary of the Reuma.pt/vasculitis contents (8).
CONCLUSION:
Let us see the advantages and limitations.
Longitudinal data involving a larger sample size, long-term efficacy, safety, ability to track natural history are a few of the strengths. Using this informations; new criteria can be developed and validated due to the huge database across various geographic regions involving many different populations.
Limitations include lack of uniformity, diversity, unavailability of complete data, and the rigorous follow-up as in trials. Duplication of data is also sometimes a drawback. There is only patient data with no controls. Large funding is needed. Trained personnel are required to feed data into electronic systems. Here the pharmaceutical industry can pitch in, as funds are huge. They can get involved in collaborations, rather than doing only their own trials. Philanthropists can also share in funding. A central force can be employed for statistics.
However, transparency is a big issue. Justice has to be rendered to every contributor to maintain the sanctity of these registries. After all the first step towards the registry is presenting a study in a conference. This has to get published in an unbiased way in order to gain entry into a registry. Numerous are precious observations that have not seen the light of the day. They could have drastically changed the outlook of a particular disease in all aspects.
Unfortunately India with its diverse population and rheumatic diseases in plenty has not come up with even a few registries, though Karnataka has made an attempt with a Rheumatoid Arthritis Registry. We are the leaders in innovative treatments in innovative doses. We can offer to the world in the best interest of the patients and science-ideas about treatment and longitudinal follow-up. All this can be made possible if there is “unity in diversity” and intra and inter-state collaborations, in an unbiased manner.
I think I have given enough food for thought to climb the mountain and hoist our flag. It's high time, we do it!!!
REFERENCES:
1. Nelly Raymond Diade.Registries in Spondyloarthritis- What have we Learned?-MOJ, Orthop and Rheumatol 2017;9(2)
2.John D.Reveille.A registry of ankylosing spondylitis registries and prospects for global interfacing.Curr opin Rheumatol 2013 Jul;25(4):468-476.
3.Astrid Rasmussen , Sidney Sevier, Jennifer A Kelly, The Family Registry And Repository Rheumatology 2011;50(1): 47-59
4.Inigo Rua-Figueroa, Francisco Javier Lopez-Longo, Jamie Calvin-Alen.National Registry of Patients with Systemic Lupus Erythematosus of the Spanish Society of Rheumatology : Objectives and Methodology . Rheumatol Clin. 2014; 10(1): 17-24
5.Manual Pombo,Suarez Iman Gomez,Reino.Role of Registry In The Treatment Of Rheumatoid Arthritis with biological DMARDS,Pharmacological Research 148 (2019) 104410.
6.Lisa G Rida,Katalin Danko and Frederick Miller. Myositis Registries and Biorepositories -powerful tools to advance clinical, epidemiological and pathogenic research. Current Opinion 2014;26:724-741.
7.Felice Galluccio,Ulrich A.Walker, Sveltana Nihtyanova. Registries in systemic sclerosis: a worldwide experience. Rheumatology 2011;50:60-68.
8.Christina Ponte, Nikita Khmelinski,Vitor Teixeira.Reuma.pt/vasculitis-the Portuguese vasculitis registry. Orphanet Journal of Rare Diseases 2020; 15: 110
Dr.S.Rajeswari M.D,D.M.
Prof & HOD, Rheumatology
Sri Ramachandra Institute Of Higher Education And Research, Porur, Chennai
